Dee Finney's blog
start date July 20, 2011
today's date June 1, 2013
page 511
ALZHEIMERS - CAUSE - PREVENTION - CURE?
WHY DOES IT RUN IN FAMILIES?
NOTE: This page came about because a friend of a friend is showing the beginning symtoms of this disease unfortunately. If there is a way to slow down the progress or even cure it, we owe it to her to try.
By Kristin Koch
Everyone struggles to come up with a name once in a while. But how can you
tell if it’s more serious?
“One symptom alone does not necessarily indicate that a person has Alzheimer’s
or dementia,” says Raj C. Shah, MD, of the Rush Memory Clinic at Rush University
Medical Center, in Chicago. (Dementia is chronic loss of cognition, usually
affecting memory, and Alzheimer’s causes 50% to 80% of dementia cases.)
There are many other causes of memory loss, including vitamin B12 deficiency,
and brain, thyroid, kidney, or liver disorders. However, having several other
symptoms could be a sign of Alzheimer’s disease (AD). Recognizing the signs of
dementia can help lead to a quicker diagnosis.
Serious memory loss and confusion are not a normal part of aging. But
forgetfulness caused by stress, anxiety, or depression can be mistaken for
dementia, especially in someone who is older.
“We all forget the exact details of a conversation or what someone told us to
do, but a person with AD will forget what just happened, what someone just said,
or what he or she just said and therefore repeat things over and over again,”
says Lisa P. Gwyther, co-author of
The Alzheimer’s Action Plan: A Family Guide.
Memory loss isn’t consistent, and people with AD may forget the dog’s name one
day and remember it the next. “Nothing is certain or predictable with most
dementias except they do progress,” says Gwyther.
It’s common for someone suffering from AD to seem anxious or agitated.
They may constantly move around and pace, get upset in certain places, or become
fixated on specific details. Agitation usually results from fear, confusion,
fatigue, and feeling overwhelmed from trying to make sense of a world that no
longer makes sense, explains Gwyther.
Certain circumstances can also make the individual more anxious, such as
relocating to a nursing home. In addition to agitation, rapid and seemingly
unprovoked mood swings are another sign of dementia—going from calm to tearful
to angry for no apparent reason.
A person with AD will begin to make decisions that seem silly, irresponsible,
or even inappropriate and are a marked departure from past behavior, such as
dressing improperly for the weather or no longer being able to assess for
themselves what is safe.
“The earliest changes in judgment usually involve money. So people who were
normally very cautious with their finances will start spending in unusual ways,
like giving money to unworthy strangers like telemarketers, or withholding money
they should pay, because they incorrectly believe their utility company is
suddenly untrustworthy,” says Gwyther.
AD sufferers have difficulty with abstract thinking as the disease
progresses, making numbers and money particularly troublesome.
While missing an occasional monthly payment isn’t something to worry about (at
least in terms of the brain’s health), if your loved one suddenly has difficulty
handling money, paying bills, managing a budget, or even understanding what
numbers represent, it could be a sign of dementia.
A person suffering from dementia often takes longer to complete, and may have
trouble finishing, everyday tasks that he or she has done hundreds of times
before.
For instance, a former whiz in the kitchen may have a problem making his or her
signature dish or even remembering how to boil water.
Common activities like remembering how to get to a familiar location, play a
favorite game, or manage a budget may also prove difficult.
As dementia progresses, your loved ones may have trouble concentrating and
find that fairly basic activities take them longer to do than before.
In particular, they may struggle to develop and follow a plan, like creating and
using a grocery list, following a recipe, or keeping track of monthly bills.
This difficultly is far more pronounced than making the occasional error when
balancing a checkbook or forgetting an item on your grocery list.
Finding car keys in the freezer, the remote in a sock drawer, or routinely
discovering other “missing” items in strange spots is usually a strong indicator
that your family member may be suffering from dementia.
Although we tend to associate forgetfulness with the natural aging process,
people with AD don’t just occasionally forget where they left their car keys or
reading glasses; they leave them in unusual places and are later unable to
retrace their steps to find them.
Often they’ll also become suspicious and accuse someone else of hiding or
stealing their belongings.
Disorientation as to time and place, such as forgetting where you live,
getting easily lost, and losing track of dates, seasons, and the passage of time
is a common experience for individuals with AD.
“The real issue with AD is perception of time,” explains Gwyther. “Five minutes
can seem like five hours for someone with AD, so a husband may think his wife
has been gone for hours or even weeks, even if it’s just been a few minutes, or
he might tell his grandchild that he hasn’t seen him in five years, even though
he just saw them yesterday.”
As dementia progresses, a person’s language and communication skills
diminish. He or she may stop mid-conversation and not know how to continue.
Vocabulary can be especially troublesome. A person may struggle to find the
right word; call things by the wrong names (e.g., a car a TV); substitute
unusual or incorrect words for familiar words and names (e.g., calling one’s
husband “him” or “that guy”); invent new words; or use familiar words over and
over again.
With time, people may rely on gestures instead of speaking, revert back to
speaking in a native language, or just speak less in general.
Unfortunately, about 60% of people with dementia have a tendency to walk off,
wander aimlessly, and become lost, often repeatedly.
Restlessness, fear, confusion related to time, the inability to recognize
familiar people, places, and objects, as well as stress can all cause wandering.
In some cases, the person might leave the house in the middle of the night to
fulfill a physical need, such as finding a toilet or food, or he may be
attempting to “go home” because he doesn’t realize he is home or he believes
it’s 20 years earlier and he needs to go to a former job.
The frequent repetition of words, statements, questions, or activities is a
hallmark of dementia and AD.
Sometimes this repetitive behavior is triggered by anxiety, boredom, or fear of
the environment or to achieve comfort, security, or familiarity.
One symptom of dementia is vision problems that are different from typical
age-related problems such as cataracts.
People with AD tend to have difficulty reading, judging distances, and
determining color or contrast as time goes on.
In terms of perception, they may look in a mirror and think someone else is in
the room instead of realizing they are looking at a reflection.
Dementia can also cause changes in visual and spatial abilities. They can find
it tough to distinguish food from the plate it’s on, for instance.
If your relative begins to routinely engage in seemingly pointless endeavors,
like opening and closing a drawer, packing and unpacking clothing, pacing, or
repeating demands or questions, it may be a sign of AD.
Although from the outside it might seem like these behaviors are futile or even
crazy, experts say they usually fulfill a need for the person, such as the need
to feel productive or busy.
AD can be a lonely and isolating disease that can result in a general lack of
interest in surrounding activities or withdrawal from family and friends. People
with AD may start to remove themselves from hobbies, social activities, work
projects, or sports they previously loved, perhaps because they forget how to
perform their favorite pastime, like knitting or playing the piano.
It’s also likely that because of all the changes they have experienced, they may
feel embarrassed or ashamed and therefore avoid social situations and friends
entirely.
If apathy, loss of interest in social activities and hobbies, and social
withdrawal occur in the early or mid-stage of AD, they may be due to depression.
About 40% of people with AD also have depression. Unfortunately, identifying
depression can be difficult, and the cognitive impairment makes it difficult for
the person to articulate his or her feelings.
If a family member sleeps all the time or watches TV all day and refuses to do
any other activities, she may have depression as well, and you should talk to
her doctor.
As AD progresses, your loved one may not always recognize you or other family
members and friends, which can be heart-breaking.
“Recognition does come and go for a while,” says Gwyther. “In general, people
forget what they just learned or whom they just met, then friends, and family
last. But sometimes it’s hard to explain why someone remembers one child’s name
and not another. Well-practiced memories and stories last longer than newer
ones, but in the very late stages, people may only remember their parents.”
Dementia affects fine motor skills, interfering with one’s
ability to button or unbutton clothes or use utensils, like
forks and knives.
But motor problems, like weakness or trembling hands, or sensory
symptoms, like numbness or loss of sensation, may also be a sign
of a different type of disease such as Parkinson’s, so it’s
important to discuss your parent’s or relative’s specific
symptoms with a doctor.
Dressing is difficult for dementia patients, who sometimes feel overwhelmed
by the choices or may not remember even how to dress, tie a shoe lace, or buckle
a belt.
They may wear the same thing over and over again, forgetting that they wore the
same outfit the day before. And as previously mentioned, buttoning and
unbuttoning clothes can become more difficult in the mid-to-late stages of AD
due to a decline in motor skills.
As the illness progresses, individuals with AD often forget to brush their
teeth, bathe regularly, change their clothes, and even use the toilet.
They may not remember why they even need to bathe or brush their teeth.
Likewise, they may forget how to comb their hair, clip their fingernails, shave,
or use a toothbrush or comb
People with dementia can literally forget to eat and drink, especially
because many AD patients experience decreased appetite and interest in food.
On the other hand, others forget that they’ve already eaten and, as a result,
eat lunch or dinner multiple times a day. Oddly enough, it’s not unusual for a
person with AD to develop new favorite foods and suddenly dislike foods he or
she previously loved.
Additionally, the person may lose the ability to tell if a food or beverage is
too hot to eat or drink, forget to chew slowly and swallow, or not remember how
to use eating utensils and revert to eating with their fingers
In the mid and especially late stages of Alzheimer’s, a person may begin to
lose control of his or her impulses and act out in inappropriate or
uncharacteristic ways.
“They may say tactless things, like ‘Gosh, you got fat,’ that they would have
never said before,” says Gwyther.
Additionally, people with AD may forget that they are married and begin to flirt
and make inappropriate sexual advances, or they might start taking their clothes
off at inappropriate times or in unusual settings.
Shoplifting is not uncommon among adults with AD, who don’t understand or
remember that they must pay for items in stores.
Some people may go from seemingly irrational suspicions (say that someone
else stole their glasses) to firmly held false beliefs or delusions (say that
someone is trying to hurt or kill them).
Additionally, they may begin experiencing hallucinations or seeing, hearing,
smelling, or tasting things that aren’t there.
A person may see the face of a former friend in a door or hear voices, for
instance. According to experts, memory loss and the ensuing confusion associated
with AD may cause the person to perceive things in new, unusual ways or become
suspicious or misinterpret what he or she actually sees and hears.
As the dementia worsens over time, it is not unusual for someone to become
physically or verbally aggressive.
Verbal outbursts, including cursing, arguing, name calling, shouting, and
threatening, are common, and some patients will even get physical, hitting and
pushing caregivers, for example.
These aggressive acts often seem to come out of nowhere, but there’s usually a
reason behind the behavior that may not be readily apparent to family members or
caregivers, such as physical discomfort, inability to communicate properly, or
frustration at a situation.
Certain symptoms, like restlessness, anxiety, agitation, disorientation, and
confusion, tend to get worse as the day goes on and even continue through the
night, often resulting in difficulty sleeping and wandering.
Experts call this phenomenon “sundowning,” and it can be due to exhaustion,
changes in the person’s biological clock, the inability to separate dreams from
reality, and a decreased need for sleep that can occur with age.
As much as 20% of Alzheimer’s patients experience sundowning at some point, and
it’s a common reason that family members decide to put their loved one in a
nursing home.
Experts refer to the tendency for AD sufferers to become completely dependent
on a certain individual and constantly follow them around as “shadowing.”
Shadowing tends to occur at the end of the day or in the evening when the person
may begin to feel particularly worn down, confused, and fearful.
“It’s often a result of getting scared in a world that is confusing to them, so
the patient constantly needs the person they most trust in view,” explains
Gwyther. “If that person is out of sight, they may not know how long they’ve
been gone or where to find them, so they will follow them around the house and
even into the bathroom.”
Even if someone has Alzheimer’s, it doesn’t mean his or her life is over; a
person with AD can live a meaningful and productive life for many years, but
it’s important to get a proper diagnosis.
People often wait too long to seek help, says Dr. Shah.
“Most diagnoses are still made in the moderate stage, after most individuals
have been experiencing symptoms for years already,” says Dr. Shah. “It doesn’t
help the person or family to wait until symptoms become so obvious that the
diagnosis can be easily made. It is better to seek an evaluation earlier to help
maintain quality of life and to prevent social or medical crises due to memory
loss.”
CAUSE OF ALZHEIMERS
Scientists believe that for most people, Alzheimer's disease results from a combination of genetic, lifestyle and environmental factors that affect the brain over time.
Less than 5 percent of the time, Alzheimer's is caused by specific genetic changes that virtually guarantee a person will develop the disease.
Although the causes of Alzheimer's are not yet fully understood, its effect on the brain is clear. Alzheimer's disease damages and kills brain cells. A brain affected by Alzheimer's disease has many fewer cells and many fewer connections among surviving cells than does a healthy brain.
As more and more brain cells die, Alzheimer's leads to significant brain shrinkage. When doctors examine Alzheimer's brain tissue under the microscope, they see two types of abnormalities that are considered hallmarks of the disease:
Scientists are still studying how plaques and tangles are related to Alzheimer’s disease. One theory is that they block nerve cells’ ability to communicate with each other, making it difficult for the cells to survive.
Autopsies have shown that most people develop some plaques and tangles as they age, but people with Alzheimer’s develop far more than those who do not develop the disease. Scientists still don’t know why some people develop so many compared to others. However, several risk factors for Alzheimer’s disease have been uncovered.
Scientists have identified two kinds of genes that are associated with this familial risk factor. The first is thought to be a “risk gene,” ApoE 4, that increases the likelihood of developing Alzheimer’s, but does not guarantee it. In addition to ApoE 4, scientists think there could be up to a dozen more risk genes yet to be discovered.
The second kind of gene is a “deterministic gene” and is much rarer than risk genes. Deterministic genes are only found in a few hundred extended families around the world. If a deterministic gene is inherited, the person will undoubtedly develop Alzheimer’s, probably at a much earlier age.
Evidence is also mounting for the promotion of exercise and a healthy diet to reduce Alzheimer’s risk. Avoiding tobacco, limiting alcohol consumption, staying socially active, and engaging in intellectually stimulating activities have also been shown to have a protective effect against Alzheimer’s disease.
Finally, there is a strong link between heart health and brain health. Those who are free of heart disease or related conditions are at a lower risk of developing Alzheimer’s or another kind of dementia than those who have cardiovascular problems.
Researchers do not know the exact cause of Alzheimer's disease, but it is most likely due to a combination of a variety of genetic and other factors. Genetic research is concentrating on the role of heredity -- the transmission of qualities and illnesses from parents to children -- in determining risk for, and development of, Alzheimer's disease.
Every healthy person has 46 chromosomes in 23 pairs. Usually, people receive one chromosome in each pair from each parent. In each chromosome, DNA forms two long, intertwined, thread-like strands that carry inherited information in the form of genes.
Genes are the basic units of heredity that can direct almost every aspect of the construction, operation, and repair of living organisms. Each gene is a set of chemical instructions that tells a cell how to make one of the many unique proteins in the body.
Genetic research has turned up evidence of a link between Alzheimer's disease and genes on four chromosomes, labeled numerically as 1, 14, 19, and 21.
The APOE gene on chromosome 19 has been linked to late-onset Alzheimer's disease, which is the most common form of the disease. Dozens of studies around the world have confirmed that inheritance of one particular variant of the APOE gene, termed APOE4, increases the lifetime risk of developing Alzheimer's disease.
One of the puzzles surrounding APOE is why some people with the APOE4 variant do not develop Alzheimer's disease and why, conversely, many people develop the disease even though they have not inherited APOE4 . APOE, in other words, although clearly influencing the risk of developing Alzheimer's, is not a consistent genetic marker for the disease.
Alzheimer's disease strikes early and fairly often in certain families, often enough to be singled out as a separate form of the disease and given a label: early-onset familial Alzheimer's disease, or FAD. Combing through the DNA of these families, researchers have found an abnormality in one gene on chromosome 21 that is common to a few of the families. And they have linked a much larger proportion of early-onset families to recently identified and related genes on chromosomes 1 and 14.
The chromosome 21 gene also intrigues Alzheimer's researchers because of its role in Down syndrome. People with Down syndrome have an extra copy of chromosome 21 and, as they grow older, usually develop abnormalities in the brain like those found in Alzheimer's disease, though often at a younger age.
Few researchers think that the search for Alzheimer's genes is over. Most investigators are convinced that there are many more genes involved in Alzheimer's disease and, moreover, that other conditions must also be present for the disease to develop. One of these conditions may be a problem with the way in which nerves turn sugar, or glucose, into energy, a process known as glucose metabolism.
Aluminum
One of the most publicized and controversial theories concerns aluminum, which became a suspect in Alzheimer's disease when researchers found traces of this metal in the brains of patients with Alzheimer's disease. Many studies since then have either not been able to confirm this finding or have had questionable results.
Important It is possible that the main title of the report Alzheimer's Disease is not the name you expected. Please check the synonyms listing to find the alternate name(s) and disorder subdivision(s) covered by this report.
Read the Alzheimer's Disease article > >
Aluminum does turn up in higher amounts than normal in some autopsy studies of Alzheimer's patients, but not in all. Further doubt about the importance of aluminum stems from the possibility that the aluminum found in some studies did not all come from the brain tissues being studied. Instead, some could have come from the special substances used in the laboratory to study brain tissue.
Aluminum is a common element in the Earth's crust and is found in small amounts in numerous household products and in many foods. As a result, there have been fears that aluminum in the diet or absorbed in other ways could be a factor in Alzheimer's. One study found that people who used antiperspirants and antacids containing aluminum had a higher risk of developing Alzheimer's. Others have also reported an association between aluminum exposure and Alzheimer's disease.
On the other hand, various studies have found that groups of people exposed to high levels of aluminum do not have an increased risk. Moreover, aluminum in cooking utensils does not get into food, and the aluminum that does occur naturally in some foods, such as potatoes, is not absorbed well by the body. On the whole, scientists can say only that it is still uncertain whether exposure to aluminum plays a role in Alzheimer's disease.
Zinc
Zinc has been implicated in Alzheimer's disease in two ways. Some reports suggest that too little zinc is a problem. Others that too much zinc is at fault. Too little zinc was suggested by autopsies that found low levels of zinc in the brains of Alzheimer's disease patients, especially in a certain region.
On the other hand, a recent study suggests that too much zinc might be the problem. In this laboratory experiment, zinc caused beta amyloid from cerebrospinal fluid -- the fluid that bathes the brain -- to form clumps similar to the plaques of Alzheimer's disease. Current experiments with zinc are pursuing this lead in laboratory tests that more closely mimic conditions in the brain.
Food-borne Poisons
Toxins in foods have come under suspicion in a few cases of dementia. Two substances found in seeds of certain legumes in Africa, India, and Guam may cause nervous system damage. Both enhance the action of a substance called glutamate, which has also been implicated in Alzheimer's disease.
In Canada, an outbreak of a nervous system disease similar to Alzheimer's occurred among people who had eaten mussels contaminated with demoic acid. This chemical, like the legume substances, enhances glutamate. While these toxins may not be a common cause of dementia, they could eventually shed some light on the mechanisms that lead to nerve cell damage.
Viruses
In some nervous system diseases, a virus is the culprit, lurking in the body for decades before a combination of circumstances stir it to action. For years, researchers have sought a virus or other infectious agent in Alzheimer's disease.
This line of research has yielded little in the way of hard evidence so far, although one study in the late 1980s did provide some data that have kept the possibility alive. A larger investigation is currently under way.
IS GENETICS A FACTOR IN ALZHEIMERS?
Scientists don't yet fully understand what causes Alzheimer's disease. However, the more they learn about this devastating disease, the more they realize that genes* play an important role in its development. Research conducted and funded by the National Institute on Aging (NIA) at the National Institutes of Health and others is advancing the field of Alzheimer's disease genetics.
*Terms in bold are defined at the end of this fact sheet.
Some diseases are caused by a genetic mutation, or permanent change in one or more specific genes. If a person inherits from a parent a genetic mutation that causes a certain disease, then he or she will usually get the disease. Sickle cell anemia, cystic fibrosis, and early-onset familial Alzheimer's disease are examples of inherited genetic disorders.
In other diseases, a genetic variant may occur. This change in a gene can sometimes cause a disease directly. More often, it acts to increase or decrease a person's risk of developing a disease or condition. When a genetic variant increases disease risk but does not directly cause a disease, it is called a genetic risk factor.
Alzheimer's disease is an irreversible, progressive brain disease. It is characterized by the development of amyloid plaques and neurofibrillary tangles, the loss of connections between nerve cells, or neurons, in the brain, and the death of these nerve cells. There are two types of Alzheimer's—early-onset and late-onset. Both types have a genetic component.
DNA, Chromosomes, and Genes
The nucleus of almost every human cell contains a “blueprint” that carries the instructions a cell needs to do its job. The blueprint is made up of DNA (deoxyribonucleic acid), which is present in long strands that would stretch to nearly 6 feet in length if attached end to end. The DNA is packed tightly together with proteins into compact structures called chromosomes. Normally, each cell has 46 chromosomes in 23 pairs, which are inherited equally from a father and a mother. The DNA in nearly all cells of an individual is identical. Each chromosome contains many thousands of segments, called genes. People inherit two copies of each gene from their parents, except for genes on the X and Y chromosomes, which, among other functions, determine a person's sex. The genes “instruct” the cell to make unique proteins that, in turn, dictate the types of cells made. Genes also direct almost every aspect of the cell's construction, operation, and repair. Even slight changes in a gene can produce a protein that functions abnormally, which may lead to disease. Other changes in genes may increase or decrease a person's risk of developing a particular disease. |
Early-onset Alzheimer's disease occurs in people age 30 to 60. It is rare, representing less than 5 percent of all people who have Alzheimer's. Some cases of early-onset Alzheimer's have no known cause, but most cases are inherited, a type known as familial Alzheimer's disease (FAD).
Familial Alzheimer's disease is caused by any one of a number of different single-gene mutations on chromosomes 21, 14, and 1. Each of these mutations causes abnormal proteins to be formed. Mutations on chromosome 21 cause the formation of abnormal amyloid precursor protein (APP). A mutation on chromosome 14 causes abnormal presenilin 1 to be made, and a mutation on chromosome 1 leads to abnormal presenilin 2.
Scientists know that each of these mutations plays a role in the breakdown of APP, a protein whose precise function is not yet known. This breakdown is part of a process that generates harmful forms of amyloid plaques, a hallmark of the disease. A child whose mother or father carries a genetic mutation for FAD has a 50/50 chance of inheriting that mutation. If the mutation is in fact inherited, the child almost surely will develop FAD.
Critical research findings about early-onset Alzheimer's have helped identify key steps in the formation of brain abnormalities typical of Alzheimer's disease. They have also led to the development of imaging tests that show the accumulation of amyloid in the living brain. In addition, the study of Alzheimer's genetics has helped explain some of the variation in the age at which the disease develops.
NIA-supported scientists are continuing this research through the Dominantly Inherited Alzheimer Network (DIAN), an international partnership to study families with a genetic mutation that causes early-onset Alzheimer's disease. By observing the biological changes that occur in these families long before symptoms appear, scientists hope to gain insight into how and why the disease develops in both its early- and late-onset forms. In addition, scientists are attempting to develop tests that will enable diagnosis of Alzheimer's before clinical signs and symptoms appear, as it is likely that early treatment will be critical as therapies become available.
Most cases of Alzheimer's are the late-onset form, which develops after age 60. The causes of late-onset Alzheimer's are not yet completely understood, but they likely include a combination of genetic, environmental, and lifestyle factors that influence a person's risk for developing the disease.
The single-gene mutations directly responsible for early-onset Alzheimer's disease do not seem to be involved in late-onset Alzheimer's. Researchers have not found a specific gene that causes the late-onset form of the disease. However, one genetic risk factor does appear to increase a person's risk of developing the disease. This increased risk is related to the apolipoprotein E (APOE) gene found on chromosome 19. APOE contains the instructions for making a protein that helps carry cholesterol and other types of fat in the bloodstream. APOE comes in several different forms, or alleles. Three forms—APOE ε2, APOE ε3, and APOE ε4—occur most frequently.
Dozens of studies have confirmed that the APOE ε4 allele increases the risk of developing Alzheimer's, but how that happens is not yet understood. These studies also help explain some of the variation in the age at which Alzheimer's disease develops, as people who inherit one or two APOE ε4 alleles tend to develop the disease at an earlier age than those who do not have any APOE ε4 alleles.
APOE ε4 is called a risk-factor gene because it increases a person's risk of developing the disease. However, inheriting an APOE ε4 allele does not mean that a person will definitely develop Alzheimer's. Some people with one or two APOE ε4 alleles never get the disease, and others who develop Alzheimer's do not have any APOE ε4 alleles.
Using a relatively new approach called genome-wide association study (GWAS), researchers have identified a number of genes in addition to APOE ε4 that may increase a person's risk for late-onset Alzheimer's, including BIN1, CLU, PICALM, and CR1. Finding genetic risk factors like these helps scientists better understand how Alzheimer's disease develops and identify possible treatments to study.
Although a blood test can identify which APOE alleles a person has, it cannot predict who will or will not develop Alzheimer's disease. It is unlikely that genetic testing will ever be able to predict the disease with 100 percent accuracy because too many other factors may influence its development and progression.
At present, APOE testing is used in research settings to identify study participants who may have an increased risk of developing Alzheimer's. This knowledge helps scientists look for early brain changes in participants and compare the effectiveness of treatments for people with different APOE profiles. Most researchers believe that APOE testing is useful for studying Alzheimer's disease risk in large groups of people but not for determining any one person's specific risk.
In doctors' offices and other clinical settings, genetic testing is used for people with a family history of early-onset Alzheimer's disease. However, it is not generally recommended for people at risk of late-onset Alzheimer's.
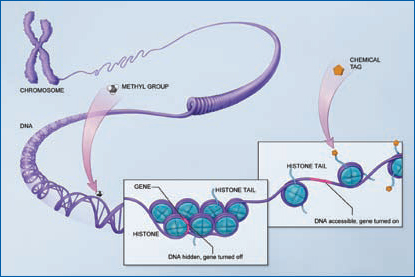
Epigenetics: Nature Meets NurtureScientists have long thought that genetic and environmental factors interact to influence a person's biological makeup, including the predisposition to different diseases. More recently, they have discovered the biological mechanisms for those interactions. The expression of genes (when particular genes are “switched” on or off) can be affected—positively and negatively—by environmental factors, such as exercise, diet, chemicals, or smoking, to which an individual may be exposed, even in the womb. Epigenetics is an emerging frontier of science focused on how and when particular genes are expressed. Diet and exposure to chemicals in the environment, among other factors, throughout all stages of life can alter a cell's DNA in ways that affect the activity of genes. That can make people more or less susceptible to developing a disease later in life. There is some emerging evidence that epigenetic mechanisms contribute to Alzheimer's disease. Epigenetic changes, whether protective, benign, or harmful, may help explain, for example, why one family member develops the disease and another does not. Research supported by the National Institutes of Health continues to explore this avenue.
The epigenome can “mark” DNA in two ways, both of which play a role in turning genes off or on. The first occurs when certain chemical tags called methyl groups attach to the backbone of a DNA molecule. The second occurs when a variety of chemical tags attach to the tails of histones, which are spool-like proteins that package DNA neatly into chromosomes. This action affects how tightly DNA is wound around the histones. |
Discovering all that we can about the role of Alzheimer's disease risk-factor genes is an important area of research. Understanding more about the genetic basis of the disease will help researchers:
Major Alzheimer's Genetics Research Efforts UnderwayAs Alzheimer's disease genetics research has intensified, it has become clear that scientists need many genetic samples to make further progress. The National Institute on Aging supports several major genetics research programs.
The participation of volunteers is a critical part of Alzheimer's disease genetics research. The more genetic information that researchers can gather and analyze from a wide range of individuals and families, the more clues they will have for finding additional risk-factor genes. To learn more about the Alzheimer's Disease Genetics Study or to volunteer, contact NCRAD toll-free at 1-800-526-2839 or visit www.ncrad.org. |
Alzheimer’s Disease
Education and Referral (ADEAR)
Center
P.O. Box 8250
Silver Spring, MD 20907-8250
1-800-438-4380 (toll-free)
www.nia.nih.gov/alzheimers
The National Institute on Aging's ADEAR Center offers information and publications for families, caregivers, and professionals on diagnosis, treatment, patient care, caregiver needs, long-term care, education and training, and research related to Alzheimer's disease. Staff members answer telephone, email, and written requests and make referrals to local and national resources. The ADEAR website provides free, online publications in English and Spanish; email alerts; a clinical trials database; the Alzheimer's Disease Library database; and more.
Additional information about genetics in health and disease is available from the National Human Genome Research Institute (NHGRI), part of the National Institutes of Health. Visit the NHGRI website at www.genome.gov.
The National Library of Medicine's National Center for Biotechnology Information also provides genetics information at www.ncbi.nlm.nih.gov.
Alzheimer's Association
225 North Michigan Avenue
Floor 17
Chicago, IL 60601-7633
1-800-272-3900 (toll-free)
1-866-403-3073 (TTY/toll-free)
www.alz.org
Alzheimer's Foundation of
America
322 Eighth Avenue, 7th floor
New York, NY 10001
1-866-232-8484 (toll-free)
www.alzfdn.org
Alzheimer’s Disease Education &
Referral (ADEAR) Center
A Service of the National Institute
on Aging
National Institutes of Health
U.S. Department of Health and Human
Services
Publication Date:
June 2011
Page Last Updated: May 21, 2013
BLOG INDEX 2011
BLOG INDEX 2012 - page 1
JANUARY THRU APRIL 2012
MAY THRU AUGUST 2012
SEPTEMBER THRU DECEMBER
BLOG INDEX 2013
BLOG INDEX - PAGE 2 - 2013